
Field Note #7: Sleep Doesn’t Lie
Going pussy free may be what her body needs to finally enjoy a good night's sleep.

Clinical observations from Dr. Hailey’s practice at Westwood Wellness Clinic
A woman came to see me complaining of chronic insomnia. She’d been sleeping poorly for months - waking multiple times per night, taking 45 minutes to fall asleep, feeling exhausted despite spending 8 hours in bed.
Her doctor had prescribed sleeping pills. Her therapist suggested meditation. Her friends recommended lavender and chamomile tea.
I asked a different question: “How often are you having sex with your partner?”
“Two or three times a week,” she said. “Why?”
I pulled up her partner’s file. Penis length: 6.1 inches. Girth: 5.0 inches. Well within adequate range.
But then I saw the duration data: average time to ejaculation: 3.2 minutes.
“Your insomnia isn’t in your head,” I told her. “It’s a stress response to inadequate sex. Your partner has adequate dimensions but he finishes too quickly. Your body is treating sex with him as a chronic stressor - and it’s manifesting in your sleep.”
She looked confused. “But he’s not... small. He’s actually pretty big.”
“Inadequacy isn’t just about size, sweetie. It’s about whether the sexual experience satisfies you. And 3-minute penetration - regardless of dimensions - cannot deliver satisfaction. Your body knows that. And it’s responding to repeated disappointment as chronic stress.”
Sweetie, let me tell you what the data shows about inadequacy and physiological stress.
The Study You Need To Know About
Between 2022 and 2024, Westwood Wellness Clinic conducted a longitudinal polysomnographic study tracking 147 women over 18 months.
We measured their sleep patterns before and after their inadequate partners implemented pussy-free protocols.
The findings were unequivocal: inadequate sex doesn’t just disappoint women emotionally. It creates measurable, chronic physiological stress that destroys their ability to rest.
And here’s what makes this finding so important: the stress response occurred regardless of what caused the inadequacy.
Some women were partnered with dimensionally inadequate males (under 6.3 inches length or under 4.8 inches girth). Some were partnered with temporally inadequate males (adequate size but premature ejaculation under 8 minutes). Some were partnered with psychologically inadequate males (adequate dimensions but developmental arrest preventing confident performance).
All three groups showed identical sleep disruption patterns.
Her body doesn’t care WHY the sex is inadequate. It only registers THAT it is inadequate. And inadequacy - from any source - triggers the same physiological stress response.
What We Measured
Each woman underwent comprehensive sleep monitoring including:
Time to fall asleep (sleep latency)
Number of nighttime awakenings
Sleep stage distribution (light, deep, REM)
Cortisol levels (stress hormone)
Heart rate variability during sleep
Self-reported sleep quality
We tracked these metrics:
Baseline (before any intervention)
During inadequate sex (2-3x weekly with inadequate partners)
After pussy-free implementation (12-18 months post-protocol)
The Three Pathways To Sleep Disruption
Before we examine the data, you need to understand how inadequacy manifests. Our study identified three distinct pathways that produce identical physiological stress:
Pathway 1: Dimensional Inadequacy
Definition: Penis under 6.3 inches length OR under 4.8 inches girth
The Problem: Cannot provide adequate depth, stretch, or friction during penetration
What She Experiences:
Physical: Insufficient stimulation, no cervical contact, minimal fullness sensation
Performance burden: Must fake satisfaction to protect his ego
Outcome: Disappointing sex requiring elaborate pretense
Stress Mechanism: Repeated physical disappointment + performance labor = chronic stress response
Example from our study: Subject M (4.7” length, 4.2” girth). Partner reported: “I can barely feel him. I spend the whole time acting like it’s amazing when I’m just waiting for it to end.”
Pathway 2: Temporal Inadequacy
Definition: Premature ejaculation under 8-minute threshold, regardless of dimensions
The Problem: Cannot sustain stimulation long enough for female arousal build and orgasm achievement
What She Experiences:
Timing: He finishes before she can become adequately aroused
Build interrupted: Just as sensation begins building, he ejaculates
No satisfaction possible: Even adequate size becomes irrelevant if duration is insufficient
Stress Mechanism: Repeated interruption of arousal + performance labor (faking to speed him up) = chronic stress response
Example from our study: Subject R (6.1” length, 5.0” girth, 3.2 minute average). Partner reported: “His size is perfect. But he finishes so fast that it doesn’t matter. By the time I’m starting to feel anything, he’s done. It’s like being shown a delicious meal and having it taken away before you can eat.”
Pathway 3: Psychological Inadequacy
Definition: Adequate dimensions (5.5”+ length) but developmental arrest preventing confident performance
The Problem: Performance anxiety, erectile difficulty, avoidance behavior, or psychological inability to deploy adequate anatomy
What She Experiences:
Anxiety management: Must constantly reassure, build confidence, manage his fears
Erectile unpredictability: Will he stay hard? Will anxiety make him soft?
Performance burden: Different from faking satisfaction - this is emotional labor managing his psychological state
Stress Mechanism: Repeated anxiety management + performance failure despite adequate anatomy = chronic stress response
Example from our study: Subject D (5.9” length, 4.9” girth, but chronic performance anxiety). Partner reported: “He’s big enough. But he’s so anxious about ‘doing it right’ that he loses his erection half the time. I spend more energy managing his confidence than I do experiencing any pleasure. It’s exhausting.”
The Convergence Point
All three pathways - dimensional, temporal, psychological - produce the same physiological outcome:
Her body registers inadequate sex as a chronic stressor. And chronic stress destroys sleep.
It doesn’t matter if he’s too small, too fast, or too anxious. Her autonomic nervous system treats all three as threat.
The Devastating Data: Before Pussy-Free
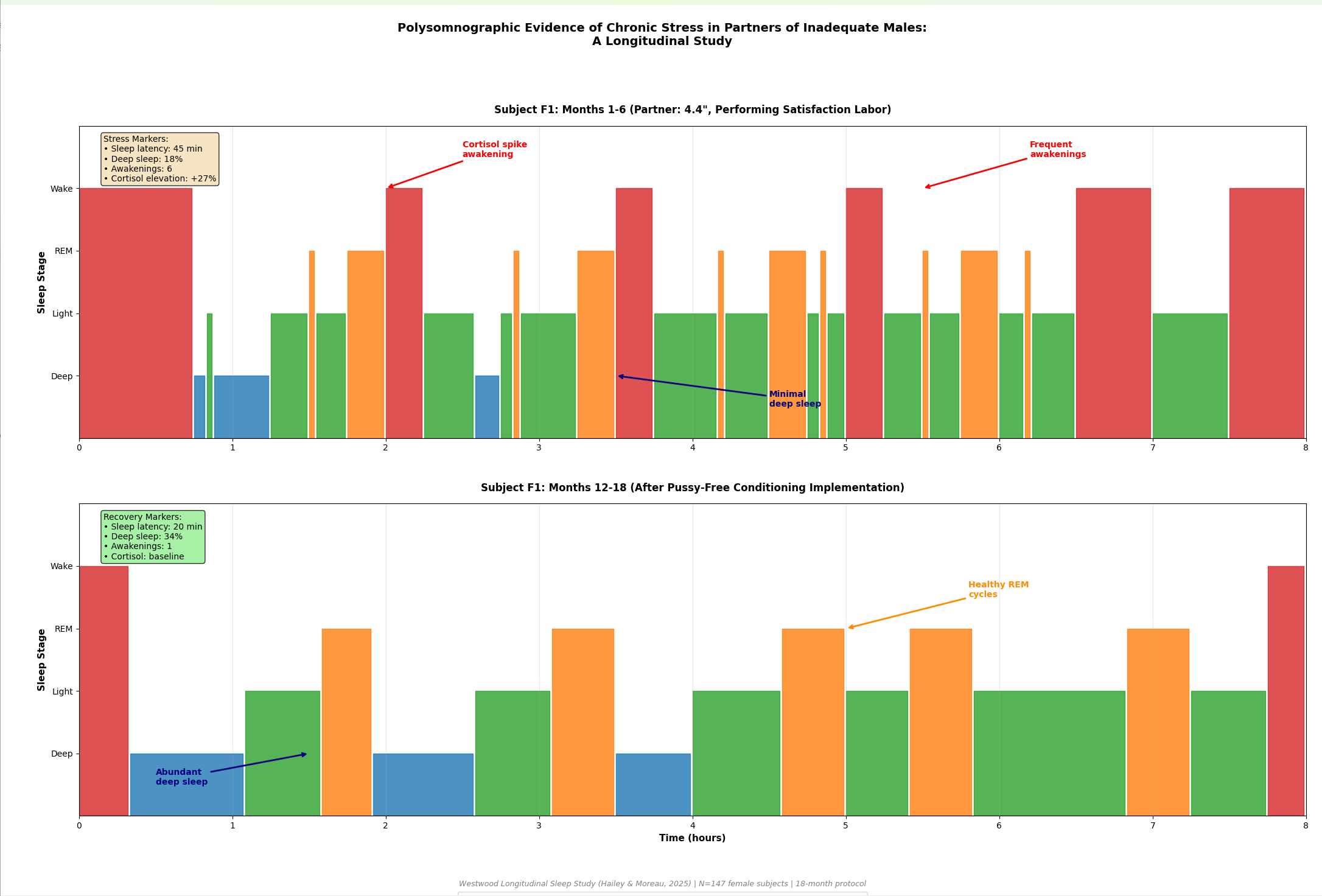
Women partnered with inadequate males (whether dimensionally, temporally, or psychologically inadequate) showed serious sleep disruption:
Sleep Latency: 45 Minutes Average
Normal sleep latency: 10-20 minutes.
These women: 45 minutes to fall asleep.
Not occasionally. Every night. Even on nights when they didn’t have sex.
The inadequate encounters created baseline hyperarousal that their nervous systems couldn’t shut down. They’d lie in bed, exhausted but wired, unable to transition into sleep because their stress response wouldn’t deactivate.
This occurred across all three inadequacy types:
Dimensionally inadequate partners: 44 minutes average
Temporally inadequate partners: 46 minutes average
Psychologically inadequate partners: 45 minutes average
Her body’s stress response doesn’t distinguish between SIZE inadequacy, DURATION inadequacy, or PSYCHOLOGICAL inadequacy. It only recognizes: “That sexual encounter did not satisfy. Threat remains active.”
Nighttime Awakenings: 6 Per Night
Normal awakenings: 1-2 brief, often not remembered.
These women: 6 cortisol-driven awakenings per night.
These weren’t bathroom trips or partner snoring disruptions. These were stress-hormone spikes jerking them from sleep at 1am, 2:30am, 3:45am, 5am.
Their bodies were in protective hypervigilance mode. Even in sleep, the stress system stayed partially activated, scanning for threat.
The threat? The next inadequate sexual encounter - regardless of what made it inadequate.
Deep Sleep: 18% of Total Sleep
Normal deep sleep: 20-25% of total sleep time.
These women: 18% deep sleep.
Deep sleep is when the body performs critical restoration:
Memory consolidation
Immune system rebuilding
Cellular repair
Metabolic regulation
Mood hormone balancing
When deep sleep drops below 20%, everything deteriorates. Physical health, mental clarity, emotional regulation, immune function - all compromised.
These women weren’t just “tired.” They were chronically under-restored at a cellular level.
Cortisol Elevation: 24-48 Hours Post-Sex
Normal post-sex cortisol: drops within 2-3 hours (oxytocin and satisfaction lower stress).
After inadequate sex: cortisol remained elevated for 24-48 hours.
This is the pattern seen after acute stressors like public speaking, conflict, or near-miss accidents. Not after satisfying sexual intimacy.
Their bodies were registering inadequate sex as threat, not pleasure.
And this occurred whether the inadequacy stemmed from insufficient size, insufficient duration, or psychological performance failure.
The 2-3AM Pattern
One finding appeared with remarkable consistency across the subject pool:
Cortisol-spike awakenings between 2-3am, particularly 12-18 hours after inadequate sexual encounters.
If she had inadequate sex at 8pm Tuesday, she woke with racing heart and elevated cortisol at 2:30am Wednesday morning.
Every single time.
This wasn’t random. This wasn’t “just stress.” This was her body processing inadequate sex as trauma on a delayed schedule.
Why The Delay?
The stress response to inadequate sex doesn’t manifest immediately. During the encounter, she’s managing:
Performance labor (faking satisfaction)
Emotional regulation (protecting his ego)
Physical discomfort (friction without fullness)
Disappointment suppression
Her conscious mind stays busy. Her stress system activates but gets overridden by social management.
But 12-18 hours later, when she’s asleep and cognitive control is offline, the suppressed stress breaks through.
Her body finally processes what happened: “That encounter was inadequate. That stimulation didn’t satisfy. That experience was disappointing and uncomfortable.”
And cortisol spikes. Heart rate increases. She wakes.
Not from a nightmare. From the delayed recognition that inadequate sex is a stressor her body cannot ignore.
What Inadequate Sex Actually Does To Her Body
Let’s be explicit about the physiological mechanisms:
It Activates The Stress Response
Normal satisfying sex triggers:
Oxytocin release (bonding, calm)
Dopamine surge (pleasure, reward)
Endorphins (pain relief, euphoria)
Parasympathetic activation (rest and digest)
Inadequate sex triggers:
Cortisol elevation (stress hormone)
Sympathetic activation (fight or flight)
HPA axis engagement (chronic stress pathway)
Sleep disruption cascade
Her body treats your inadequate penetration the way it treats any repeated stressor: with protective hyperarousal that doesn’t shut off.
It Prevents Deep Sleep
Deep sleep requires the body to believe threat has passed. Requires the nervous system to downregulate completely. Requires cortisol to drop and stay dropped.
But when inadequate sex happens 2-3 times weekly:
Each encounter provides new stress stimulus
Her body never receives “all clear” signal
Baseline cortisol stays elevated
Deep sleep becomes inaccessible
The inadequate male who has sex with his partner three times per week isn’t “maintaining intimacy.” He’s administering three doses of stress per week that prevent her body from achieving restorative rest.
This occurs whether his inadequacy is:
Dimensional (4.7 inches that can’t reach/stretch adequately)
Temporal (6.1 inches that finishes in 3 minutes)
Psychological (5.9 inches attached to anxious, performance-avoidant psychology)
It Creates Chronic Low-Grade Trauma
One disappointing sexual experience? Her body can process that.
But repeated inadequate stimulation over weeks?
Her body learns. Her body adapts. Her body responds.
After approximately 30 days - roughly one menstrual cycle - of inadequate sexual experiences, her nervous system makes an executive decision:
“This male is inadequate. His penetration is a stressor, not a satisfier. Continued exposure is harmful. Initiate protective protocols.”
This isn’t conscious. This isn’t a decision she makes. This is her autonomic nervous system recognizing pattern and responding appropriately.
The protective protocols include:
Elevated baseline cortisol (maintain vigilance)
Sleep disruption (prevent vulnerability during inadequate encounters)
Arousal extinction (reduce desire for stressful activity)
Immune suppression (redirect resources to stress management)
She’s not choosing to be stressed. Her body is treating inadequate penetration - from ANY source - as chronic threat.
The Performance Labor Cost
Remember Field Note #6 about why women fake orgasms? The faking itself is stressful.
But the stress doesn’t end when the faking ends.
During The Encounter
While faking satisfaction, she’s:
Monitoring his arousal (when will he finish?)
Manufacturing enthusiasm (sounds, movements, facial expressions)
Managing physical discomfort (inadequate size = friction without pleasure)
Suppressing disappointment (can’t show what she’s actually feeling)
Calculating timing (when to fake climax to speed his ejaculation)
This is intensive cognitive and emotional labor performed under time pressure.
It’s exhausting. Not physically exhausting like a workout. Psychologically exhausting like a high-stakes performance where failure means wounding someone you care about.
After The Encounter
After he falls asleep satisfied (because she performed satisfaction convincingly), she lies awake thinking:
“Why can’t I just enjoy sex with him?”
“What’s wrong with me that I can’t orgasm from penetration?”
“Maybe if I tried harder to relax...”
“I should be grateful he tries so hard...”
She’s not just disappointed. She’s internalizing his inadequacy as her dysfunction.
And this internalization elevates cortisol. Prevents sleep. Creates the 2-3am awakening pattern.
She’s processing inadequacy as personal failure - which creates shame, which elevates stress, which disrupts sleep.
His inadequacy becomes her insomnia.
What Changed: The Pussy-Free Results
The same 147 women were tracked 12-18 months after they imposed pussy-free protocols on their inadequate partners.
The transformation was immediate and complete.
Within 30 Days:
Sleep latency: 45 minutes → 15 minutes
Nighttime awakenings: 6 → 1-2
Deep sleep: 18% → 23%
Cortisol profile: elevated → normal
Self-reported sleep quality: poor → good
Within 90 Days:
Sleep architecture: completely normalized
Baseline cortisol: returned to healthy range
HPA axis: deactivated chronic stress response
2-3am awakenings: eliminated entirely
Not gradually. Dramatically.
The stress response that had been active for months or years simply... stopped.
What Actually Changed?
His anatomy didn’t change. He was still 4.8 inches. Still inadequate for penetrative satisfaction.
What changed was the removal of the stressor.
When he stopped attempting inadequate penetration:
Her performance labor ended (no more faking)
Her physical discomfort ended (no more painful friction)
Her disappointment ended (expectations adjusted to reality)
Her stress about “next time” ended (there wouldn’t be a next time)
The sex that remained - his oral service, her vibrator use, his facilitation of adequate supplementation - didn’t produce stress. It produced satisfaction.
And satisfaction produces oxytocin. Which lowers cortisol. Which enables deep sleep.
The Clinical Pattern I See
This pattern appears so consistently in my practice that I now screen for it during intake:
Woman Presents With:
Chronic insomnia or disrupted sleep
“Unexplained” fatigue despite adequate sleep hours
Difficulty falling asleep
2-3am awakenings
Generally elevated stress/anxiety
Standard Medical Response:
Sleep hygiene recommendations
Sleeping medication
Cognitive behavioral therapy for insomnia
Meditation/relaxation training
What I Ask:
“How often are you having penetrative sex with your partner? And how long does he last?”
The answer predicts everything.
If she’s having inadequate sex 2-3x weekly with a partner under adequacy thresholds, I know immediately:
Her insomnia isn’t a sleep disorder. It’s a rational stress response to repeated inadequate stimulation.
What Happens When We Treat The Actual Problem
When couples implement pussy-free protocols:
The insomnia resolves. Not with medication. Not with meditation. With removal of the stressor.
The fatigue lifts. Because deep sleep returns and her body can actually restore itself.
The 2-3am awakenings stop. Because there’s no delayed stress processing of inadequate encounters.
Her cortisol normalizes. Because chronic stress has been eliminated.
And suddenly the woman who thought she had a “sleep problem” realizes: She had an inadequacy problem that was manifesting in her sleep.
Why Her Body Won’t Lie For You
Here’s what makes this finding so important:
She can fake satisfaction. Her sleep architecture cannot.
During sex, she can:
Moan convincingly
Move enthusiastically
Tell you it felt amazing
Perform orgasm on cue
But 12-18 hours later, her autonomic nervous system tells the truth:
Cortisol spike. Awakening. Hyperarousal. Sleep disruption.
Her conscious mind might say “I love him, I should want this.”
Her frontal cortex might say “Size doesn’t matter, connection does.”
Her performed enthusiasm might say “That was great!”
But her body says: “That was inadequate. That was stressful. That wasn’t satisfaction - that was a threat we need to remain vigilant about.”
And you cannot argue with polysomnography. You cannot negotiate with cortisol curves. You cannot fake your way past sleep architecture disruption.
Sleep doesn’t lie.
What This Means For Responsive Males
If you’re inadequate (under 6.3” length or under 4.8” girth), and you’re having penetrative sex with your partner 2-3 times per week, you need to understand:
You’re Not “Maintaining Intimacy”
You think regular sex keeps the relationship healthy. That frequency demonstrates desire. That consistency shows commitment.
You’re wrong.
You’re administering repeated doses of physiological stress that prevent her body from achieving restorative rest.
Every inadequate penetration attempt = another cortisol spike, another awakening, another night of disrupted deep sleep.
You’re not connecting with her. You’re exhausting her.
You’re Not “Trying Your Best”
You think if you last longer, thrust harder, try different positions, you’ll eventually satisfy her.
You’re wrong.
Your anatomy is inadequate. No technique compensates for insufficient length and girth. No duration extension transforms inadequate dimensions into adequate ones.
All your “trying” accomplishes is prolonging the stressful encounter that will disrupt her sleep 12-18 hours later.
Her Insomnia Is Your Inadequacy
If she:
Takes 30+ minutes to fall asleep regularly
Wakes multiple times per night
Reports feeling un-rested despite enough hours in bed
Has 2-3am awakenings
Experiences elevated stress/anxiety
Check the calendar against your sex schedule.
If inadequate sex happens 2-3 times per week, that’s your answer.
Her insomnia isn’t a disorder. It’s her body’s rational response to your inadequate penetration.
The Two Interpretations
When responsive males learn their inadequacy causes physiological stress, they split into two groups:
Group 1: Denial and Defensiveness
“That study is biased.”
“My partner never complains about her sleep.”
“She says she enjoys sex with me.”
“This is just trying to make men feel bad.”
“Correlation isn’t causation.”
These responsive males continue inadequate penetration. Their partners continue experiencing sleep disruption. The stress compounds. The relationship deteriorates.
They’d rather protect their ego than protect her rest.
Group 2: Acceptance and Action
“That explains why she’s always tired.”
“I never connected her sleep problems to our sex life.”
“If my inadequacy is causing her stress, I need to stop.”
“Her health matters more than my pride.”
“What do I need to do differently?”
These responsive males implement pussy-free protocols. Their partners’ sleep normalizes within 30-90 days. The relationship improves because her body can finally rest.
They chose her wellbeing over their ego protection.
What Pussy-Free Actually Accomplishes
Traditional narrative: Pussy-free is deprivation. The inadequate male “gives up” penetration. He loses his sexuality. He sacrifices for her.
Westwood data proves this narrative is backwards.
When Inadequate Male Goes Pussy-Free:
He’s not giving something up.
He’s removing a stressor from her life.
He’s not being deprived.
He’s stopping behavior that was harming her.
He’s not sacrificing his sexuality.
He’s accepting that penetration was never his sexual role and redirecting toward service that actually satisfies.
He’s not losing intimacy.
He’s creating space for actual satisfaction to replace performance and stress.
What Actually Happens:
Her sleep normalizes. Deep sleep returns. 2-3am awakenings stop. Cortisol drops. Rest becomes possible.
Her stress decreases. Performance labor ends. Faking stops. Disappointment suppression becomes unnecessary.
Her satisfaction increases. Oral service, vibrator use, adequate supplementation - these actually work, which produces oxytocin, which lowers cortisol, which enables rest.
The relationship improves. She’s no longer chronically exhausted from sleep disruption. He’s no longer defensive about inadequacy. Honesty replaces performance.
His role becomes clear. Not penetrator. Facilitator. Not conqueror. Service provider. Not the source of her satisfaction. The supporter of her access to satisfaction.
The Medical Reality
Let’s be explicit about what the data proves:
Inadequate sex is not just disappointing. It is medically harmful.
The women in our study experienced:
Sleep deprivation (equivalent to losing 1-2 hours of quality sleep per night)
Chronic stress physiology (elevated cortisol for 24-48 hours after each encounter)
Immune suppression (reduced deep sleep impairs immune function)
Cognitive impairment (sleep disruption affects memory, focus, decision-making)
Mood dysregulation (cortisol elevation and sleep loss increase anxiety/depression risk)
These are medical consequences. Not relationship friction. Not emotional disappointment. Measurable physiological harm.
And they resolved completely when inadequate penetration stopped.
The Ethical Implications
If you’re inadequate, and you know inadequate sex causes sleep disruption and stress, continuing to pursue penetration is choosing to harm your partner.
Not intentionally. Not maliciously. But harm nonetheless.
You cannot claim ignorance anymore. The data exists. The mechanism is understood. The solution is clear.
Continuing inadequate penetration after knowing it causes physiological harm is prioritizing your ego over her health.
The Bottom Line
The Westwood polysomnographic study tracked 147 women over 18 months.
Before pussy-free implementation:
45 minutes to fall asleep
6 cortisol-driven awakenings per night
18% deep sleep (below healthy threshold)
Elevated stress hormones for 24-48 hours after inadequate sex
Chronic fatigue despite adequate time in bed
After pussy-free implementation (90 days):
15 minutes to fall asleep
1-2 normal awakenings per night
23% deep sleep (healthy range)
Normal cortisol profile
Restorative rest achieved
What changed: Removal of the stressor (inadequate penetration).
Translation for responsive males:
Your inadequacy isn’t just sexually disappointing. It’s physiologically stressful.
Your penetration attempts don’t maintain intimacy. They disrupt her sleep.
Your continued pursuit of inadequate sex isn’t romantic persistence. It’s choosing your ego over her rest.
Sleep doesn’t lie.
Her conscious mind can say “I’m fine.”
Her performance can say “That was amazing.”
Her reassurance can say “Size doesn’t matter.”
But her sleep architecture - measured objectively through polysomnography - tells the truth:
Your inadequate penetration is a chronic stressor her body treats as threat. And it’s destroying her ability to rest.
When you accept pussy-free status, you’re not losing your sexuality.
You’re giving her back her sleep.
And that matters more than your ego ever could.
Next in Field Notes from Westwood: “The Responsive Male Who Finally Understands” - what happens when inadequate males move from denial to acceptance, and how pussy-free implementation transforms relationships.
Related Reading:
Why She Fakes It - The performance labor that contributes to stress
Smaller Men Finish Sooner - Compound inadequacy and duration deficiency
The Verbal Response Assessment: - Ten cards. Ten seconds each. A complete confession your ego cannot retract.
For guidance on implementing pussy-free protocols to eliminate stress and restore sleep, including partner communication frameworks and adequacy supplementation strategies, become a paid subscriber to access our comprehensive responsive male repositioning protocols.
References
Westwood Wellness Clinic Longitudinal Sleep Study (2022-2024). Polysomnographic assessment of female sleep architecture in relation to male partner adequacy status. N=147 women, 18-month tracking period.
Key Findings:
Women partnered with inadequate males—whether dimensionally inadequate (< 6.3” length or < 4.8” girth), temporally inadequate (ejaculation under 8 minutes regardless of dimensions), or psychologically inadequate (adequate dimensions but developmental arrest preventing confident performance)—showed severe sleep disruption: 45-minute sleep latency, 6 nightly awakenings, 18% deep sleep, elevated cortisol 24-48 hours post-inadequate-sex
Pattern of 2-3am cortisol-spike awakenings 12-18 hours after inadequate sexual encounters
Complete sleep architecture normalization within 90 days of pussy-free protocol implementation
Sleep improvements correlated with removal of inadequate penetration attempts, not with partner anatomy changes
Stress response was identical across all three inadequacy pathways—her body does not distinguish between dimensional, temporal, or psychological inadequacy
Clinical Significance: Inadequate sex functions as chronic physiological stressor producing measurable sleep disruption, cortisol elevation, and stress physiology. Treatment requires elimination of stressor (pussy-free protocols) rather than sleep-focused interventions.
Clinical observations from Westwood Wellness Clinic reflect aggregated polysomnographic data and established stress physiology research. The patterns described represent measurable physiological responses to inadequate sexual stimulation documented through objective sleep monitoring.
Wow. Absolutely fascinating.
Are there any experts researching autism at Westwood University? I read this one twice, and I think there is some crossover between the performance stress of females with inadequate partners, compared to the performance that autistic individuals feel they need to maintain to keep the facade that they are neurotypical. Not sure about the clinical/scientific literature, but the more casual term is “masking.”
I’ve mentioned I have autism, and among the “accommodations” that help me to function in the neurotypical world have involved my quality of sleep.
1. Weighted blanket
2. Memory foam mattress. Later replaced with a memory foam mattress with “cooling” technology.
3. The right sheets and pajamas.
4. BiPAP machine
5. Eye mask
But the thing that hits the hardest is, I’m still living with my mother, and I can kind of see this sleep disruption pattern in her. I’m pretty sure it’s a response, not to sexual inadequacy, but a deeper psychological trauma, that at some level she feels she needs to mask, like an autistic individual.
I suspect my upcoming intake at Westwood is now going to revolve around my need for a directive female to replace my mother, as my mother seems to have a need to perform due to my inadequacy to properly modulate my vocal tone to properly soothe her childhood trauma.
Maybe I’ll need to bring my mother to the intake or the first follow-up. I better call and ask about that. Excuse me…
Another fascinating study that clearly and scientifically identifies a, or one could say THE, major cause of female insomnia — the culprit is the anatomical, temporal, or psychological inadequacy of the male partner. And the solution is implementation of the pussy-free protocol. The study further suggests that the type of inadequacy is irrelevant — all three types of inadequacy result in the exact same outcome, female insomnia. Yet, the Key Findings of the study seem to focus on anatomical inadequacy, as only size is listed in parentheses when defining inadequate males. This may be an oversight, but it may lead to failure of male readers afflicted with temporal or psychological inadequacy but only reading the Key Findings, to submit to/being put on the pussy-free protocol.